
Nikolai Kazantsev (IfM, University of Cambridge)
The response to the COVID-19 pandemic demonstrated significant difficulties in producing vital healthcare equipment, including ventilators. As the probability of another virus outbreak is expected to reach 27% in the next decade, it is crucial to develop manufacturing capabilities for initiating emergency production with greater speed, efficiency, and cost-effectiveness. In this article, Nikolai Kazantsev from the Institute for Manufacturing (IfM) at the University of Cambridge suggests three steps to building pandemic preparedness. He draws on their recent study which offers insight into how UK manufacturers can navigate uncertain periods and contribute to critical public health initiatives.
Takeaways:
- During a pandemic, it is necessary to reconfigure supply chains for emergency production.
- Preparedness can be facilitated through three key steps:
- Identifying products and components necessary to fulfil human needs.
- Mapping manufacturing capabilities across supply chains for a potential response.
- Developing an AI model to triage production options when the pandemic starts.
- Government investment in pandemic preparedness will prevent delays, improve quality, and reduce recovery costs.
Preparing for future pandemics
The UK’s National Risk Register (2023) has identified a future pandemic as one of the five most probable catastrophic risks. Future pandemics could have critical negative impacts on human health, particularly cardiac and digestive health, with the potential to disrupt water and food systems. With the World Health Organization continuing to discuss the potential of unknown diseases of high contamination and mortality that can trigger a pandemic worldwide (a so-called ‘Disease X’), novel efforts are needed to prepare the manufacturing sector for future emergency production.
Up to now, most of the focus on pandemic preparedness has been on developing vaccine technology platforms for future virus strains and antibiotics for bacteria, especially considering the threat of antimicrobial resistance. However, what has been neglected is the local manufacturing capabilities to produce the quantity and variety of supplies required to deal with pandemic impacts. These capabilities should be able to meet potential production needs and guarantee that every patient in need of medical equipment can access it even during the peak of a crisis.
Emergency product designs must be safe to use and fit for purpose rather than complex and stylish. It is also essential to learn how to triage existing manufacturing capabilities at the outset of any pandemic outbreak, considering quality, lead times, and production scale-up costs. Moreover, emergency production planning should consider the risks of individual factory disruption and related component scarcity. The aim is to facilitate the development of supply chains capable of responding to the likely or quasi-certain emergence of demand and fluctuations therein for emergency products beyond those previously produced within supply chains.
Case study: Emergency consortia across supply chains
Ventilator production in the UK during COVID-19 has produced much knowledge of scaling up emergency equipment. In March 2020, the Cabinet Office identified the urgent need to manufacture healthcare ventilators to support critically ill patients’ breathing functions. Working in collaboration with clinicians and the Medicines and Healthcare Products Regulatory Agency, they developed the specifications for the Rapidly Manufactured Ventilator System. Because no single company could handle the emergency production on its own, this could have been overcome only through consortium effort. Emergency consortia are networks ‘wider’ than existing supply chains, which aggregate various capabilities to respond to unmet demand during disruptions that have a broad resonance, such as pandemics. Consortia are built around the required product components (e.g. a bill of materials for ventilator production) and often include companies that are non-traditional to the medical industry, such as aerospace and automotive manufacturers, technology providers, manufacturers, and third-party logistics firms.
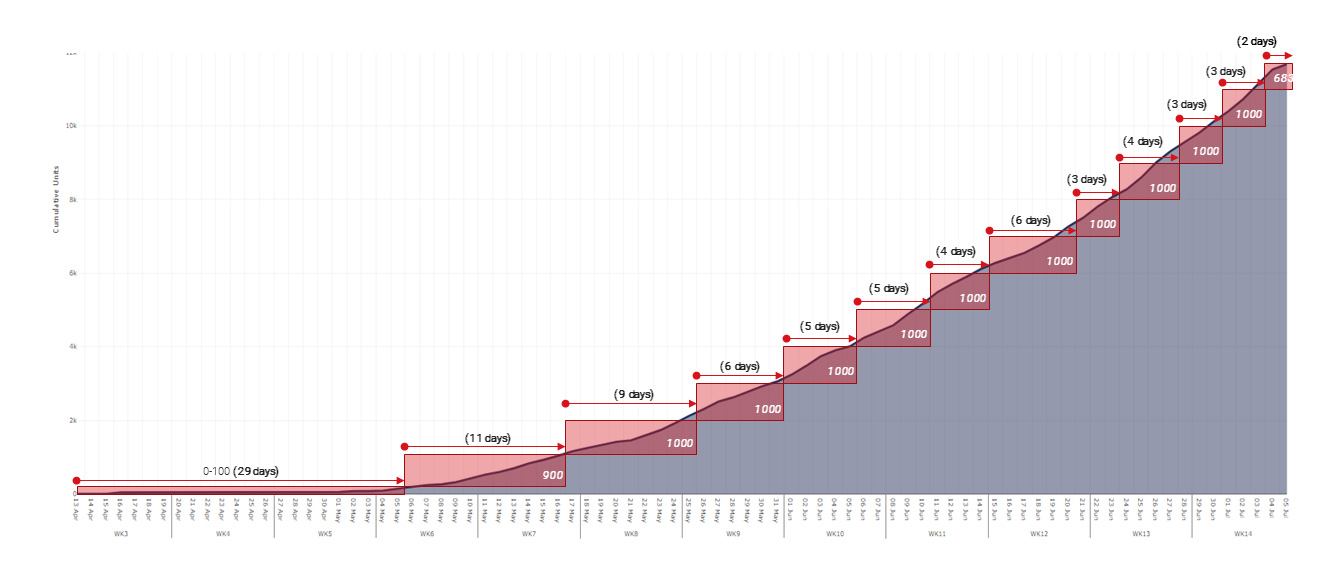
For example, ‘Ventilator Challenge UK’ (VC UK) consortium was an example of a massive achievement that produced in 12 weeks over half of all the ventilators made available to the NHS during the pandemic. Focused on a desire to save lives, VC UK led the way in digital innovation, leveraging technology such as a digital twin of the production process, simulation of production facilities, and the use of “augmented reality” glasses to train 3,500 assembly workers, all while adhering to strict social distancing measures. From VC UK’s success, one still has much to learn about how to plan emergency production faster, better, and cheaper in the eventuality of another pandemic. For example, as there was no approved emergency product design, the first 29 days of the project were spent on redesigning the similar product (anaesthesia machine) to meet the functionality and safety scale-up needs of the ventilator specification. Moreover, this redesign faced multiple bottlenecks at the component level that limited the pace of emergency production scale-up and required continuous constraint optimisation.
{kind=link}
Building a process of future pandemic preparedness
Based on the case study, three steps for manufacturers have been suggested: (1) identifying products and components necessary to fulfil human needs; (2) mapping UK manufacturing capabilities across supply chains to deploy capacity for these products; (3) developing a tool to triage options when the pandemic starts.

- Production needs
According to the ‘Futures Wheel’ toolkit, recommended by the Government Office for Science, a pandemic is an example of an event that creates cascading causal effects. While a pandemic can take various forms, the population will need similar functions, such as preventing contamination (the direct consequences of that risk), supporting primary care (‘second order’) or sustaining critical human functions within intensive care (‘third order’ consequences). For example, first, second and third-order consequences of the pandemic risk bring the following production needs:
- Need to prevent contamination: PPE, water filters, sanitisers, and disinfectants.
- Need to support primary care: vaccines and antibiotic medicine.
- Need to support intensive care: ventilators and other ICU equipment.
Design and production specialists/ physicians and hospital experts should confirm what equipment and designs will be needed in any epidemic affecting patients’ vital functions. However, it is not enough simply to identify emergency products. These products must be certified as fit-for-purpose during a future pandemic, ensuring safety and quality, and adaptability in the expectation of potential shortages. Paradoxically, the better 1st order emergency production (for preventing contamination), and 2nd order production (primary care), the less one would need (far more) complex 3rd order emergency production.
Moreover, building similar consequences after other risks from the National Risk Register and overlapping production needs can help prioritise production preparedness covering the greatest number of risks.
- Manufacturing capabilities
A rapid roll-out of emergency products requires capabilities to deploy manufacturing capacity close to demand. Recent evidence from the US suggests that systematic investments in a combination of local inventories, manufacturing capacities, and capabilities produce the best response to the pandemic. Hence, the potential emergency products and their components should be mapped with the existing list of inventories, capacities, and manufacturing capabilities. That will facilitate simulations of demand for emergency equipment driven by potential pandemics and calculations of the number of emergency products manufactured to meet this (the lead time of ‘Ventilator Challenge UK’ production during COVID-19 was three months). For example, if there is a demand for 30,000 cardio stimulators – How quickly can this be satisfied locally, i.e., without reliance on imports? What would be the lead time/costs? The outcomes can be presented using technology such as the augmented reality platforms (industrial metaverse), to better interpret and explain these simulations.
To improve emergency production results, preparatory efforts must include identifying similar products and equipment, in addition to developing cross-disciplinary skills across large firms’ medical and engineering specialisms that may be reused for emergency production. Smaller firms must be supported in undergoing certification protocols to become regular suppliers to the NHS through their normal procurement framework.
- Triage options
The future pandemic is expected to impact various parts of global supply chains, particularly in densely populated regions. Unfortunately, predicting which factories within supply chains will be disrupted and which components might become unavailable is impossible. However, under pandemic conditions, most companies, especially those in unaffected areas, are likely to be willing to help. As new manufacturing capabilities become available, efforts should focus on developing an adaptable AI model to align existing capabilities with risks and offer practical solutions to address supply chain bottlenecks for emergency production.
Such a model can base on the AI tools, which helps match production needs with manufacturing capabilities and can suggest new connections between components. By integrating manufacturing capabilities for emergency product, AI can help to infer real options across supply chains after the pandemic starts and arrange those considering costs, lead time, or carbon dioxide emission. For example, AI tool can suggest alternative inventories, factories, or even supply chains for the specified product design to deliver a scarce component, define the best response, and reduce the number of consortia working in parallel. For example, one can use stress testing, a method developed by David Simchi-Levi from the MIT Data Science Lab, to identify significant risks in a supply chain. This method helps find small but important component suppliers that may become bottlenecks in the supply chain when demand changes and it improves overall supply chain resilience.
Improving local manufacturing capabilities
While the COVID-19 experience suggests the rationale for running multiple teams in parallel to manage risks of non-delivery, an excessive number of teams working in parallel drains resources, overloads regulatory bodies, and increases recovery costs. As an alternative, the development of local manufacturing capabilities would make a significant difference in improving production resilience in the UK by enabling current supply chains to be reconfigured for human necessities. Moreover, with the advancement in AI, having an adaptable AI model capable of handling the triage at a state of readiness could be a powerful national asset. It can demonstrate the production readiness for potential demand shocks, such as the future pandemic. Policymakers might test it using real industrial intervention, increasing confidence that the population will be safe.
The UK Cabinet Office should consider updating resilience and innovation policies, considering the risks identified in the National Risk Register (2023), to formalise activating production consortia at the onset of the next pandemic and strengthen long-term supply chain resilience. These include: Responding to Emergencies, theNational Resilience Framework, the Resilience Capabilities Programme and the Supply Chain Resilience Framework.
What practical steps should manufacturers take to prepare?
- Focus on ‘known unknowns’; identify where you fit in to support emergency production.
- Register participation in the local resilience forums (LRFs) and consider extending business strategy with risk and resilience.
- Enable regular stress testing of the supply chain, considering potential bottlenecks to production growth.
The IfM is currently working on developing elastic manufacturing systems for highly regulated sectors such as aerospace, automotive, and food. These industries have very strict regulations, which limit production agility. The goal is to support the operation of UK manufacturers under continual demand fluctuations.
If you would like to collaborate with the team regarding pandemic preparedness, please contact Dr. Nikolai Kazantsev — nk622@cam.ac.uk or IfM Engage (ifm-enquiries@eng.cam.ac.uk).
Acknowledgement: The article is devoted to the 4th anniversary of ‘Ventilator Challenge UK’ consortium. The author acknowledges Dick Elsy, CBE, the former Chief Executive Officer of the High Value Manufacturing Catapult (HVM Catapult), for feedback on the paper development, and the kind help and inspiration of Elizabeth Garnsey, Professor Emerita, IfM, University of Cambridge and the community of Clare Hall College. This work was supported by the UKRI Made Smarter Innovation Challenge and the Economic and Social Research Council via InterAct [Grant Reference ES/W007231/1]. Further, the first author acknowledges EPSRC funding, grant reference EP/T024429/1 via ‘Elastic Manufacturing systems – a platform for dynamic, resilient and cost-effective manufacturing services’.